The patient, a 55-yo-female, presented to the ED with acute onset upper abdominal pain. Her PMH was unremarkable and she had no known history of prior abdominal procedures, stones, masses, peptic ulcer disease or any chronic abdominal pain. On exam, vitals were stable. However, she was found to have tenderness to palpation in the RUQ. Screening lab work revealed an elevated lipase >1000 with a mild WBC.
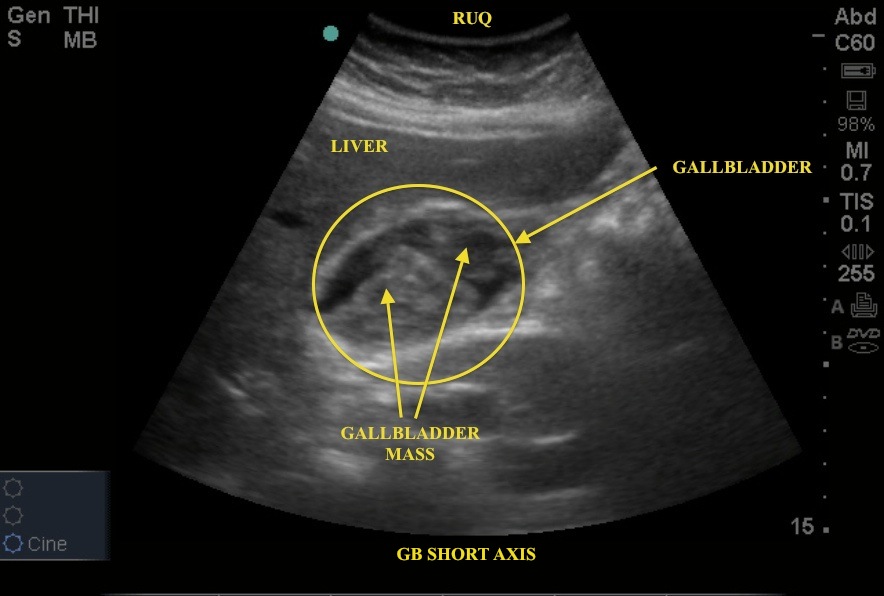
Appropriately thinking GB pathology, the curvilinear probe was used to evaluate the RUQ. See Image 1 - Gallbladder in short axis. Note the spherical GB with contents of mixed echogenicity.
Image 1
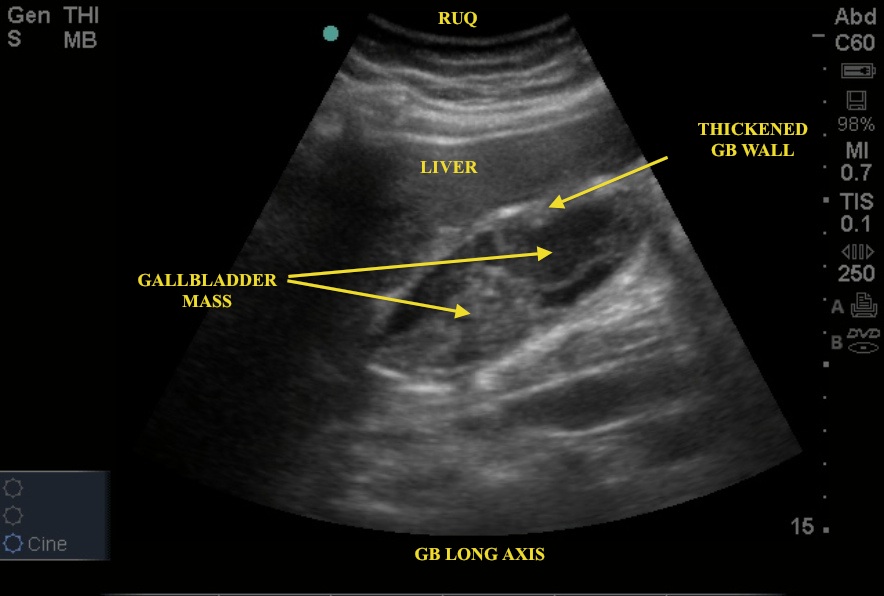
In Image 2 - Gallbladder in long axis - note a similar picture to the short axis view with the addition of a thickened GB wall and similar contents of mixed echogenicity. A quick glance may make you think that the hyperechoic contents is biliary sludge or perhaps even a GB stone - neither being correct. Look closely to see that contents do not layer out in a dependent fashion, nor is there any posterior shadowing. Further review of the imaging suggests that the "sludge" in this image is most consistent with soft tissue, likely representing a neoplastic process.
Image 2
This patient was admitted to general Surgery pending additional imaging of the abdomen for presumed GB carcinoma. Her case illustrates a subtle but excellent bedside US finding that could easily have been mistaken for another diagnosis.