The IOW this week comes from Dr. Hany Atallah and involves various images, both US related and not.
In brief, the pt arrived tachy, SOB, and pleuritic CP. Hx of HIV, CD4 count of 2, and recent admission to the hospital for prior infectious workup of similar presentation.
Let's take the ED evaluation through the following images and think of your DDx as you see each one.
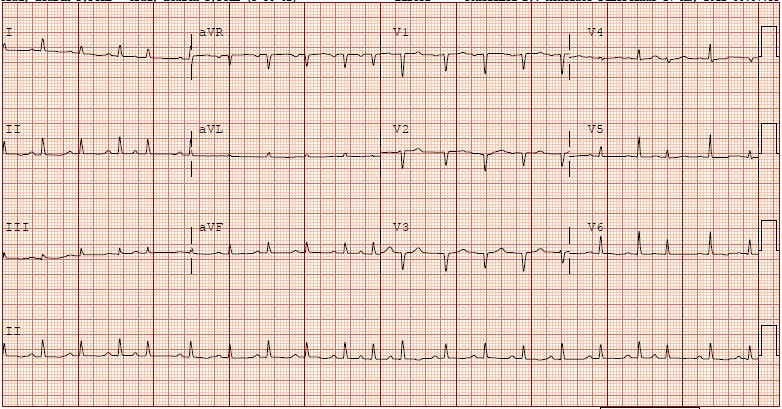
EKG
CXR
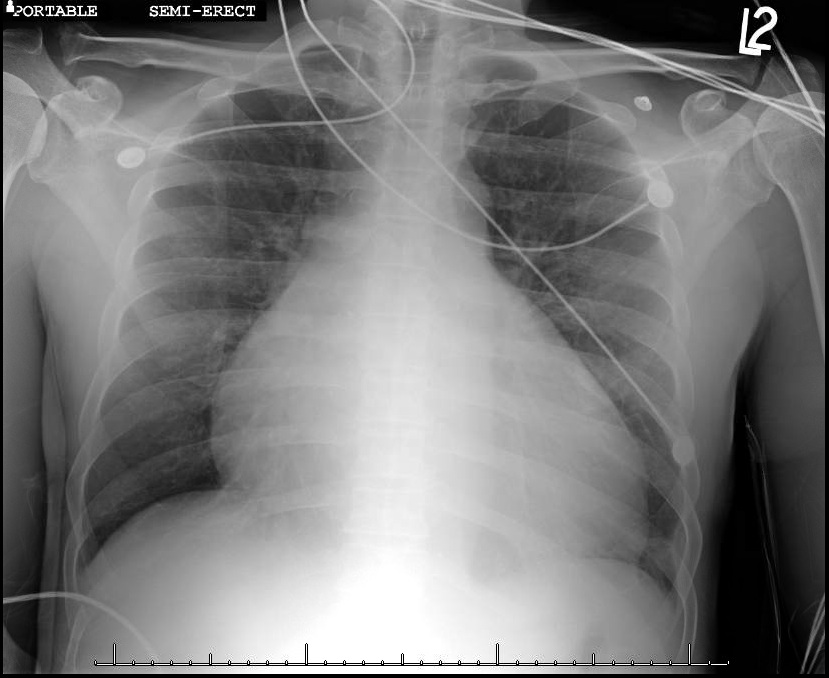
What are you thinking based on these images? The EKG shows a classic finding, that when placed alongside the CXR should get you to the bedside stat with the US.
What was noticed? What do you expect the Echo to show?
Bedside Cardiac US
In all these cardiac views notice the significant pericardial effusion and the swinging of the heart about its base. The EKG shows the classic findings of a pericardial effusion - electrical alternans. You can see it well in the chest leads V5 & V6. The globus nature of the heart on the CXR should also make you think of pericardial effusion vs a dilated cardiomyopathy. The US is diagnostic - of interest, look at the PSLA and PSSA images closely - not the bowing in of the RV this is NOT NORMAL and is a textbook finding of sonographic tamponade. Recall Beck's triad of distended neck veins, distant heart sounds, and HYPOtension. This pt was teetering on HYPOtension and the decision was made to tap the effusion with cardiology in the ED. A total of 1200cc of fluid was removed with improved MAPs. The pt was admitted, is doing better, and is a few days s/p OR for a pericardial window.
Date: May 2012