Image of the Fortnight is focusing on small bowel obstruction cases
Two Emory EM residents were looking for a bowel obstruction using ultrasound last month. They found … frankly, a whole lot of nothing.
This is mainly a bunch of air and some blood vessels that you don’t need to pay attention to right now. Both large and small bowel usually have a lot of air within and overlying them, and so normal bowel does not typically show up at all with ultrasound.
With an attending, an EM resident saw a young man with no chronic medical issues or prior abdominal surgeries who presented with constipation for 10 days. He was still passing gas, but he began vomiting the day of his ED visit. Aside from mild tachycardia, vital signs were normal. They found him moderately distended on exam, and proceeded with a bedside ultrasound to evaluate for signs of bowel obstruction.
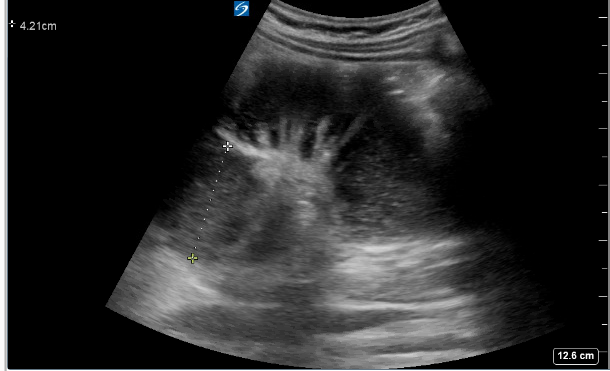
He met all the sonographic criteria for small bowel obstruction:
- 3 or more dilated loops of bowels
- Bowel dilation >2.5cm
- Alternating (bidirectional) peristalsis (luminal contents cannot keep moving forward due to obstruction)
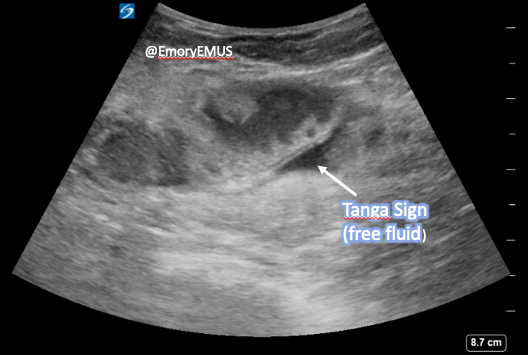
He also had a "tanga sign," a (usually triangular) collection of free fluid interspersed between bowel loops. This is a transudative phenomenon of bowel wall edema and connotes high grade obstruction (and therefore worse prognosis).
He was transferred to the care of a surgical team.
The last case was from a middle-aged patient whose paracentesis an Emory EM doctor was asked to supervise.
That is a collection of fluid, but it is contained within bowel. There is debris within it, and there are visible plicae circulares with alternating peristalsis. The bowel loops were ~4.5cm (extra big).
Look again.
This patient also went on to a hospital course involving an ICU stay.
Pearls:
- For most of these you will want to use the curvilinear ("big"/abdominal) probe, unless your patient is very thin (or a child), where you may be able to get away with using the linear (vascular) probe.
- This ultrasound exam is almost foolproof because the technique only requires you to "lawnmower" your way across all 4 quadrants of the abdomen.
- Sensitivity is about 90% so use this as a rule-in test.
- You will need to save both images (measurement of bowel loops) and clips (videos to document peristalsis).
- Keep your hand still when recording/observing peristalsis.
Consider particularly for:
- Constipated patients who have vomiting, appreciable distension, or otherwise appear ill
- Recurrent SBO patients who get multiple CTs/year
Most of these patients will end up with a CT anyway (aside from the perhaps the patient with prior adhesive SBO with recurrent/typical symptoms who responds to non-operative care). The surgical team will typically want at least a plain film on record. Ultrasound can help you triage patients for advanced imaging.
Please note, ultrasound can’t tell you:
- If this is an ileus vs. an adhesive or mechanical obstruction
- Where the transition point is
Thanks to Drs. Rahel Gizaw and Daniel Freeman for drafting this edition.
May your alcohol-based hand sanitizer and your soap dispensers never be empty.
Tricia A. Smith, MD, MPH
Assistant Professor
Department of Emergency Medicine
Emory University School of Medicine