This week the IOW is from an evaluation of a patient with SOB and tachycardia. The EM physician used dedicated cardiac views to narrow the differential.
Do you see an effusion? Does the EF look normal? Is there chamber enlargement? What should you be thinking about these views? See labeled still images #1 and #2.
Image 1
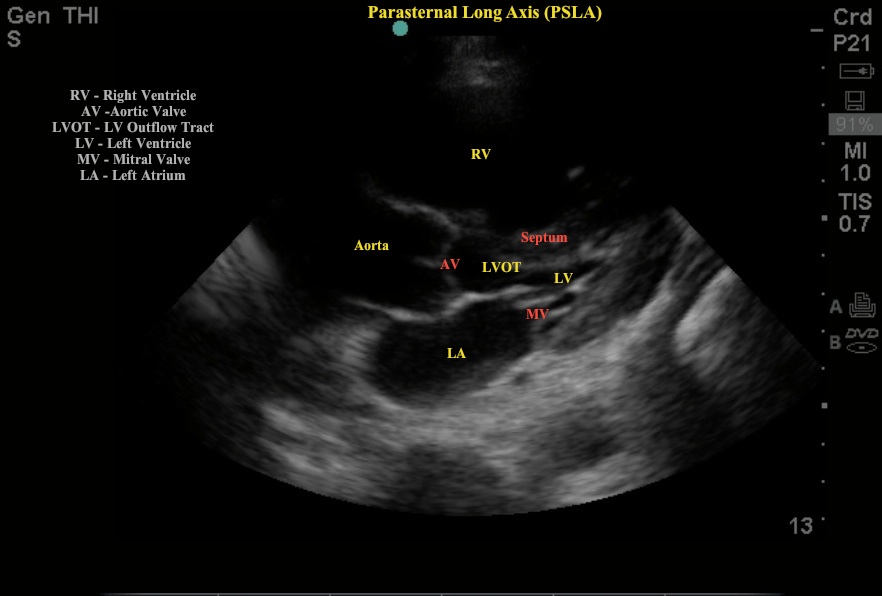
Image 2
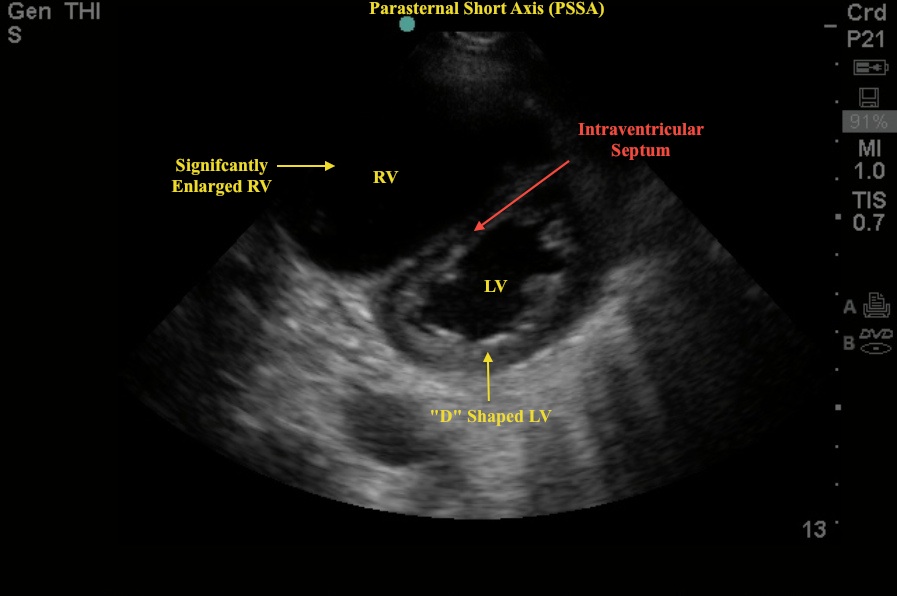
This patient had concerning vital signs (elevated HR and RR) and also had significant risk factors to suspect Acute PE (metastatic cancer, prior PE). On the PSLA view note the LARGE RV and atypical movement of the intra-ventricular septum into the much smaller LV. In the PSSA view note again the LARGE RV and the "D" shape of the LV. During right heart strain, the inter-ventricular septum flattens and makes the PSSA view of the left ventricle look like the letter “D” instead of the letter “O”.
These images are from a patient with CHRONIC right heart failure, not acute right heart strain from a PE. The take-home is that these two diagnoses can have similar bedside echo findings. An enlarged RV alone does not confirm the diagnosis of a PE. The clinical context and any prior workups (previous echos) may be your best guide. The following bedside echo findings MAY suggest the diagnosis of hemodynamically significant PE:
- “D” sign as noted above
- Enlarged RV to LV Ratio
- A right free ventricular wall <0.4cm in diameter
- A McConnell's sign - right ventricular strain with normal apical right ventricular function
Date: 2012