Cardiac sonography is best performed using the phased array probe. The most commonly used ED views include subxiphoid, parasternal, and apical 4-chamber. The technique for obtaining these views is discussed in the prior image of the week discussions. ED bedside echocardiography is best performed with focused clinical questions in mind. Usually, these questions seek to answer if there is an effusion, how is the ejection fraction, and/or is there any evidence of right heart strain.
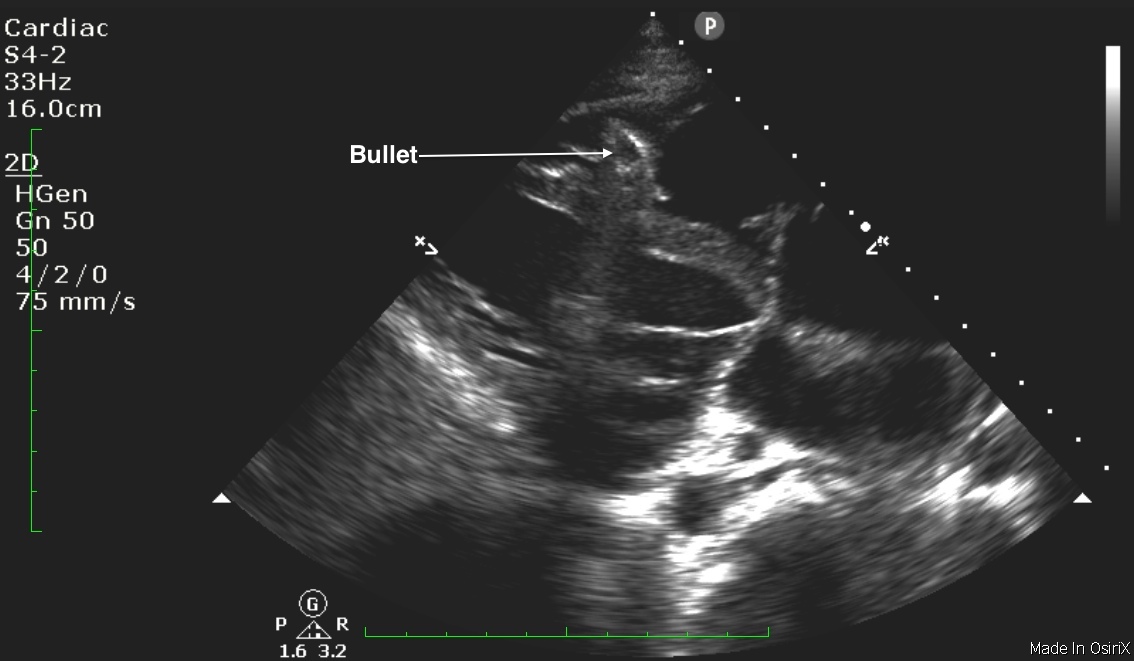
One of our EM doctors answered an unusual question: is there a foreign body lodged in the myocardium? His patient with penetrating trauma had a recent sternotomy with the repair. However, a bullet was left intact for fear of further iatrogenic damage from retrieval attempts. Using bedside ultrasound, the doctor demonstrates a bullet fragment lodged in the myocardium. Most foreign bodies will cast a posterior shadow as deeper ultrasound beam penetration is obstructed. Metallic foreign bodies, in addition, are also hyperechoic.
Image 1: Midline Still Photo
Clinical Importance: Detection of a soft-tissue foreign body is common yet often difficult, particularly when the foreign material is not radiopaque. Various imaging modalities have been advocated for detecting foreign bodies that are not revealed by plain radiography. The use of ultrasound for the detection of foreign bodies is not a new technique: it has been successfully employed for decades to facilitate bedside detection and retrieval. The article below discusses the abilities of plain radiography, xerography, computed tomography, and ultrasonography to detect glass, wooden, and plastic foreign bodies in an in vitro preparation. The authors conclude that while all these imaging techniques demonstrated a glass foreign body, only ultrasonography clearly identified wooden and plastic foreign bodies.
Literature Support: Ginsburg et al. Detection of soft-tissue foreign bodies by plain radiography, xerography, computed tomography, and ultrasonography. Annals of EM, 1990.
Date: 2014