This week's image of the week is brought to us by Dr. Gina Porter. She used an ultrasound-guided ulnar nerve block to facilitate the reduction of a 5th metacarpal (Boxer's) fracture. Her patient presented with hand pain and swelling after a fight.
Image 1
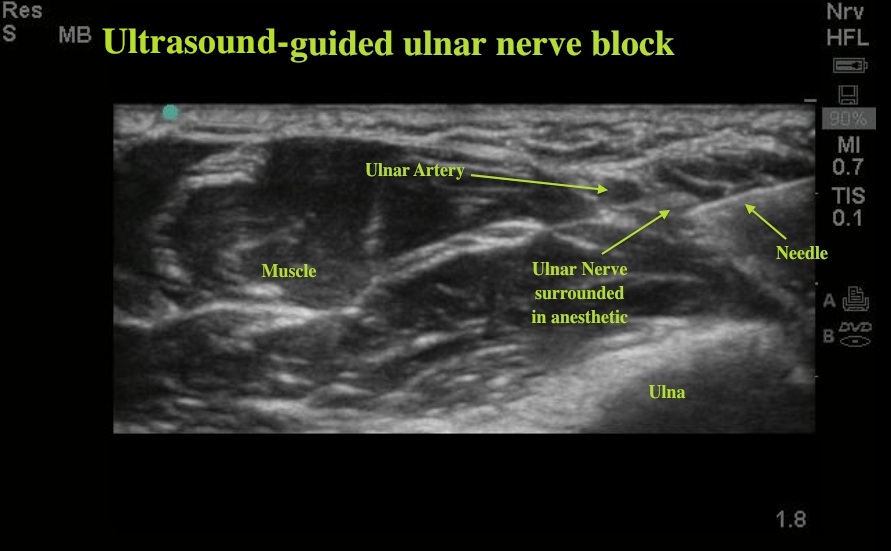
Image 2
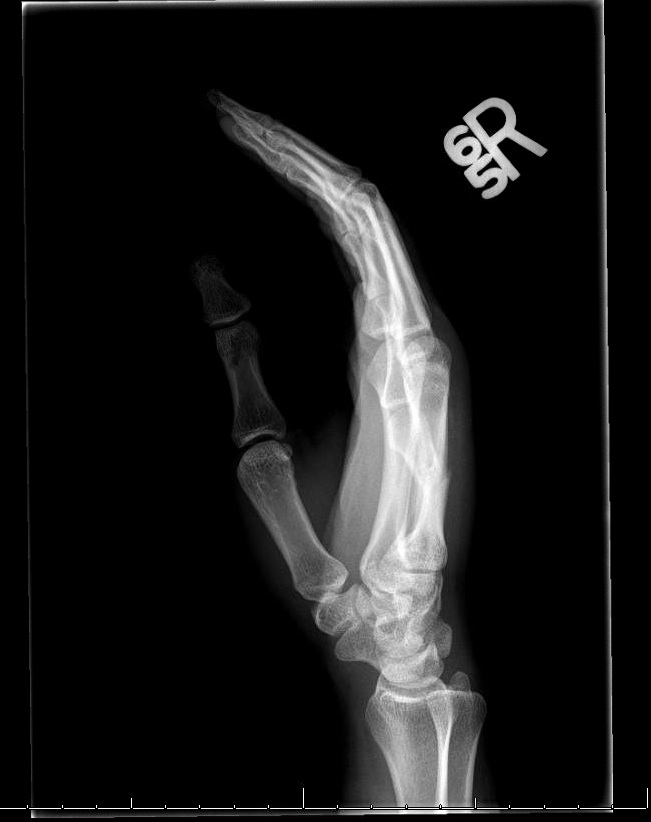
Image 3
 X-rays showed a 5th MC fracture with 60 degrees of palmar angulation. On exam, there was "scissoring" of the fingers on passive flexion indicating rotational deformity. Both findings are indications for reduction. Typically these fractures are reduced using a hematoma block, but an ulnar nerve block can provide more effective anesthesia to the area. Nerves will typically appear hyperechoic (bright) relative to surrounding soft tissues. In cross-section, nerves look like a bundle of small cables. At the wrist, the ulnar nerve will run on the ulnar side of the ulnar artery. Scanning on the palmar side of the wrist, the nerve can be traced proximally until it separates from the artery. In this image we see the needle entering in-plane on the screen. The goal is to get close to the nerve so that it is bathed in anesthetic, but not inject directly into the nerve sheath. If the needle touches the nerve the patient will report paresthesias shooting to the small and ring fingers, and the needle should be withdrawn a few millimeters. This patient had excellent anesthesia and the fracture was reduced to near anatomic alignment.
X-rays showed a 5th MC fracture with 60 degrees of palmar angulation. On exam, there was "scissoring" of the fingers on passive flexion indicating rotational deformity. Both findings are indications for reduction. Typically these fractures are reduced using a hematoma block, but an ulnar nerve block can provide more effective anesthesia to the area. Nerves will typically appear hyperechoic (bright) relative to surrounding soft tissues. In cross-section, nerves look like a bundle of small cables. At the wrist, the ulnar nerve will run on the ulnar side of the ulnar artery. Scanning on the palmar side of the wrist, the nerve can be traced proximally until it separates from the artery. In this image we see the needle entering in-plane on the screen. The goal is to get close to the nerve so that it is bathed in anesthetic, but not inject directly into the nerve sheath. If the needle touches the nerve the patient will report paresthesias shooting to the small and ring fingers, and the needle should be withdrawn a few millimeters. This patient had excellent anesthesia and the fracture was reduced to near anatomic alignment.
Date: September 2012