The IOW this week comes from Drs Deutsch, Holmes, and Almehbash. They placed an ultrasound-guided subclavian central line in the midtown ED last week. Ultrasound guidance has been shown to increase success rates and decrease rates of complications in comparison to traditional landmark guided techniques for subclavian access. You may also see this referred to as an ultrasound-guided axillary line, as the vein is typically accessed near the point where the axillary vein crosses the 1st rib and becomes subclavian.
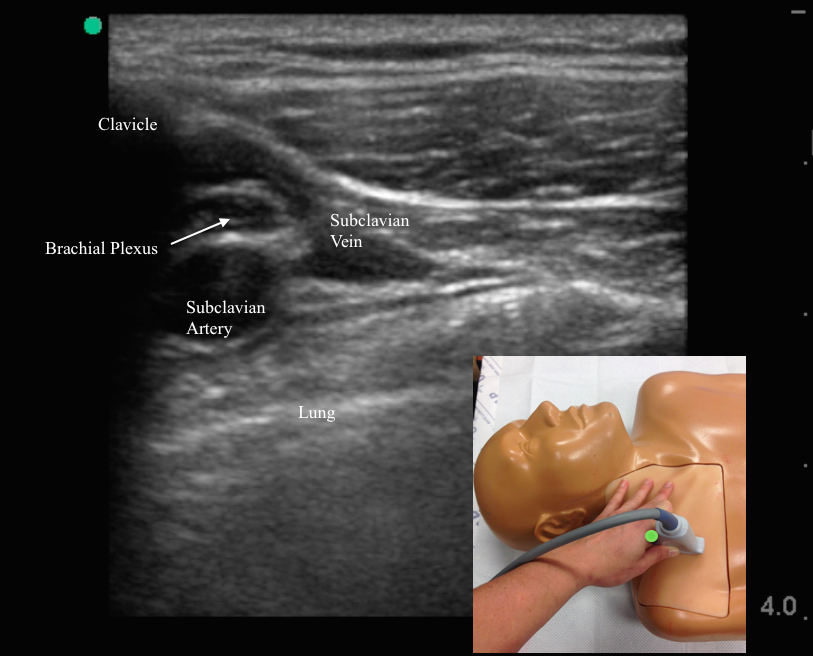
To do this procedure, first, the ultrasound probe is placed with the indicator marker pointed towards the patients head so the vein is seen in a short-axis orientation. This view allows you to identify the vein and distinguish it from the subclavian artery and brachial plexus. Compression or Doppler imaging can help you to distinguish the artery from the vein.
Image 1
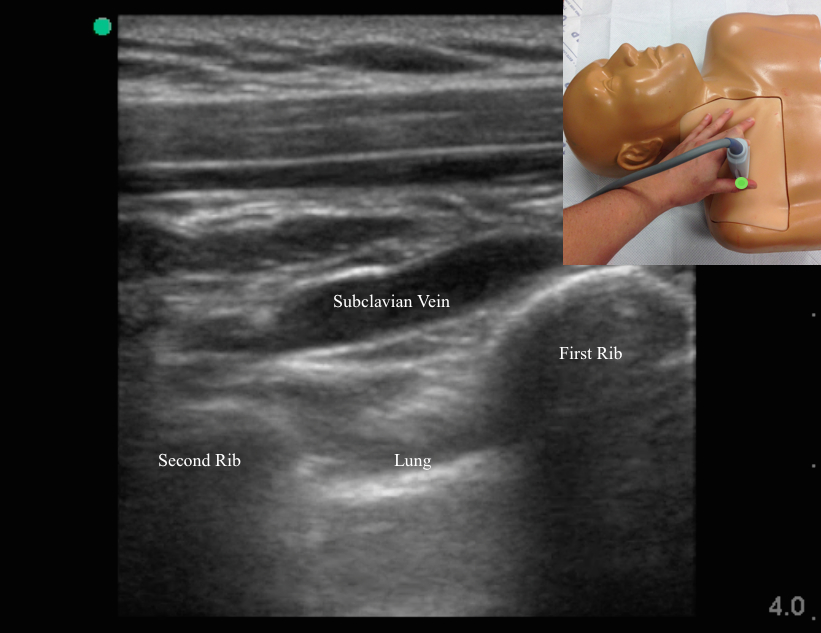
Once you have identified the vein, place it in the center of the image and slowly rotate the probe approximately 90 degrees so the indicator marker is pointed towards you and the vein is seen in a long axis orientation (Image2). Confirm again that you are visualizing the vein and not the artery.
Image 2
The vein is cannulated using an in-plane technique so the entire track of the needle can be visualized as it approaches the vein. For added safety try to aim to contact the vein where it overlies the first or second rib to decrease your chances of causing a pneumothorax. Here's the ultrasound of their line placement.
Further reading: Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: a prospective randomized study. Fragou M, et al. Critical Care Medicine. 2011 Jul;39(7):1607-12.