Images come from a case seen in the Marcus Trauma Center. The treatment team included Drs Schrager, Ragwar, Rosa and Meer. A 22-year-old female competitive gymnast was brought in after "horsing around" with her boyfriend. She had a clinically apparent patellar dislocation of Rt leg and was in severe distress. She continued to have severe pain despite IV doses of narcotics. She was offered a choice between procedural sedation or regional anesthesia. The patient elected for an ultrasound-guided nerve block. Pre- and the post-block neurovascular exam was documented. A femoral nerve block was placed and the nerve was surrounded with 20 cc 1% lidocaine under ultrasound guidance. The block was successful and the patella was successfully and easily reduced without complications. The patient was observed for a brief period of time with neuro checks and discharged home with a knee immobilizer and crutches. She was also given the Orthopedic clinic follow up.
Background
US-guided nerve blocks are both rapid and effective for pain relief and facilitating painful procedures.
Indications for femoral nerve block
- Femoral neck fractures
- Femur shaft fractures
- Patellar injury
- Large laceration/abscess over the anteromedial thigh
Contra-indications for femoral nerve block
- Intoxicated, altered mental status, or uncooperative patient (barrier to performing pre- and post-block neuro exam)
- Diabetes (higher risk population for potential nerve injury)
- Infection at the site of injection
- The risk for compartment syndrome (lose the ability to perform neuro exams temporarily)
Patient Preparation
- Place the patient on a cardiac monitor
- Select high-frequency transducer and place adhesive barrier dressing over it
- Draw up 20 cc of 1-2% lidocaine in the syringe and attach 3.5 inch 20G spinal needle
Scanning and Injection Technique
- Image the femoral vessels and nerve at the inguinal crease in the transverse plane
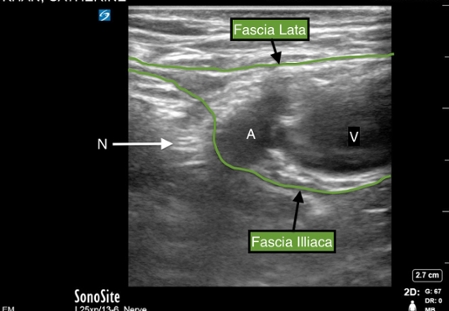
- The femoral nerve will be lateral to the femoral artery (Image 1)
- Note hyperechoic fascia layers (lata and illiaca)
- In order for the anesthetic to spread and surround the nerve, the needle needs to be deep to fascia iliaca.
- The needle is inserted using an in-plane technique so the shaft and tip of the needle can be visualized (Video 1)
- Advance the needle slowly 1-2 cm at a time, direct needle to the lateral edge of femoral nerve, aspirate to check for inadvertent vascular puncture, and inject 1 cc anesthetic
- If the fluid is not visualized on screen, stop injecting and move the probe to find needle tip (Video 2)
Complications
- Peripheral nerve injury - Rare when using US guidance. Suspect intraneural injection if the patient complains of painful paresthesias or high injection pressures are required. Re-position and re-inject
- Compartment Syndrome - Theoretical concern that femoral nerve block can delay the diagnosis of compartment syndrome. No case reports found in the literature.
- Local Anesthetic Systemic Toxicity (LAST) - Rare with US guidance, a potentially life-threatening complication when large volumes of anesthetic injected inadvertently in intravascular space, Rx ACLS procedures, drug, and lipid emulsion therapy.
Image 1
Ultrasound image of inguinal/femoral area showing vein (V), artery (A) and femoral nerve (N). The nerve will appear as a circular hyperechoic structure with a honeycomb pattern. Note the 2 fascial planes that need to be penetrated by a needle for successful femoral nerve block: first, fascia lata and second, fascia illiaca.