Dr. Taylor demonstrates a quick and easy way to confirm appropriate central line positioning using bedside ultrasound.
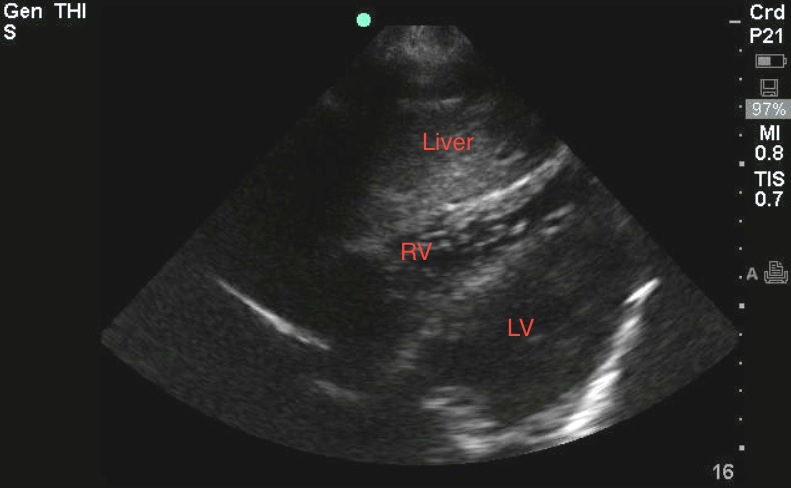
By rapidly flushing agitated normal saline (9ml saline and 1ml air) in one central line port while your ultrasound probe is positioned over the heart, you can visualize that your catheter tip is in the correct position. Venous placement is indicated by the laminar flow of bubbles seen in the right ventricle. Use the subxiphoid view to evaluate whether the tip of your catheter is in the RA, RV or IVC, or if your line is too deep. To obtain the subxiphoid view, place the curvilinear or phased array probe in the subxiphoid region with probe marker oriented to patient’s right, using the liver as an acoustic window. Although contrast ultrasound (agitated saline) does give slightly more information, it is not necessary to identify the catheter tip in the heart. If you can see the tip, it is easy to pull the line back.
Image 1
Clinical Importance
Central line placement confirmation has traditionally be done using CXR. Ultrasound provides an easy, accurate, and timely alternative. Use the ultrasound probe to help you locate the vessel, insert your needle, and confirm guidewire placement and catheter tip position. This technique can also be used to assist in floating a transvenous pacer wire.
Literature Support
Vezzani et al. used contrast-enhanced cardiac ultrasound (used agitated saline) to create microbubbles which will appear as turbulent flow through the vessel (see video above) to further demonstrate catheter tip position. This study described a concordance with CXR of 95% for catheter tip misplacement and 98% for pneumothorax. Ultrasound localization of central vein catheter and detection of postprocedural pneumothorax: An alternative to chest radiograph: Vezzani et al.: Crit Care Med 2010 Vol. 38, No. 2
Date: July 2013