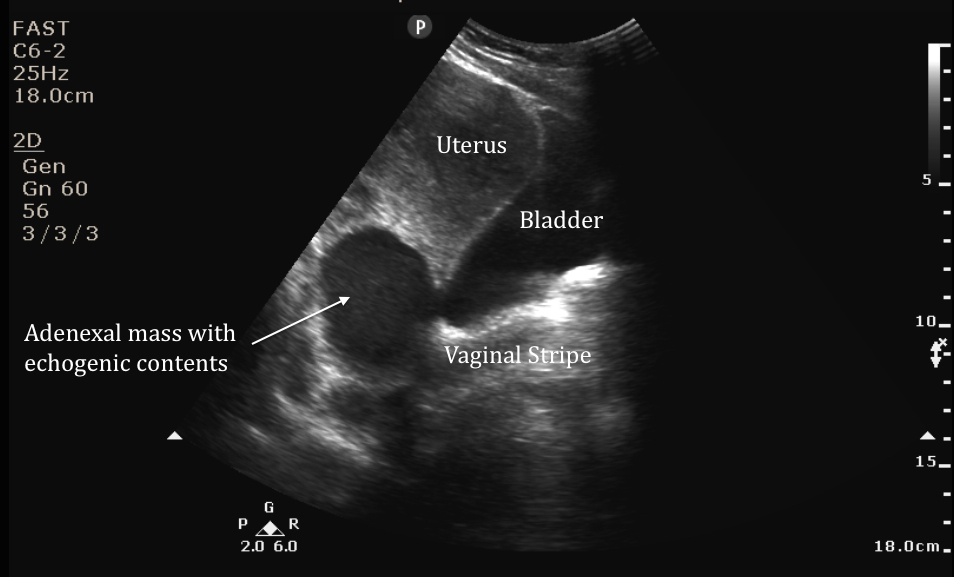
Images come from Dr Rutz, who identified large adnexal mass on bedside ultrasound. His patient was a middle-aged woman who presented with persistent pelvic pain despite recent oral antibiotic therapy for PID. To begin the scan the probe was placed with the indicator marker pointed towards the patient's head with the probe in the midline so a sagittal view of the uterus could be obtained. As he fanned to the side (Image 1), a small adnexal mass with echogenic contents was seen posteriolateral to the uterus.
Image 1
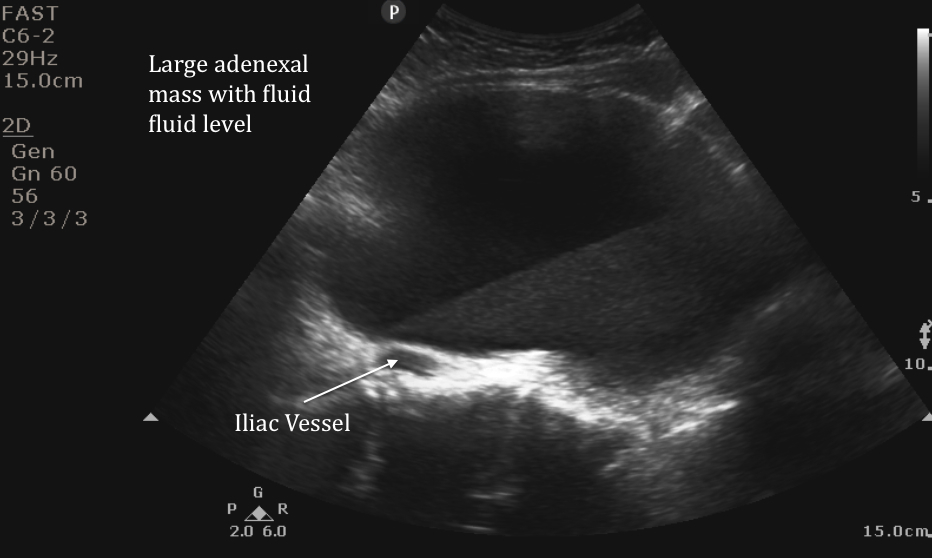
Then sweeping to the other adnexa, the image below was obtained. Note the presence of a fluid pus level that can be seen in this large cystic mass. This can often be seen with pyosalpinx or tubo-ovarian abscess. TOAs can take on a variety of appearances. Some may be located, have irregular or thick-walled borders, and typically contents are echogenic. Clinical history is important as TOA can be difficult to distinguish from other adnexal masses. Blood within hemorrhagic cysts may appear similar to pus.
Image 2
The majority of patients with tubo-ovarian abscesses can be managed with IV antibiotics alone. If there is suspicion for rupture, the patient is hemodynamically unstable, or has signs of an acute abdomen, emergent surgery is indicated. Abscesses <9cm in diameter can typically be managed with IV antibiotic alone. Those with larger fluid collections or inadequate response to antibiotic therapy may require drainage. This patient underwent CT-guided drainage of the larger mass with aspiration of 700cc of pus, received IV antibiotics and was discharged after an uneventful hospital course.
Date: September 2014