The IOW this week comes from Dr. Katie Dean. The pt, a 21-year-old, sexually active G3P2, presented to the ER with lower abdominal pain, cramping and passing large clots this AM while showering. Vitals stable with GYN exam significant for passage of clots. Quickly-performed bedside pelvic ultrasound revealed the following case video below.
Image 1
 .
.
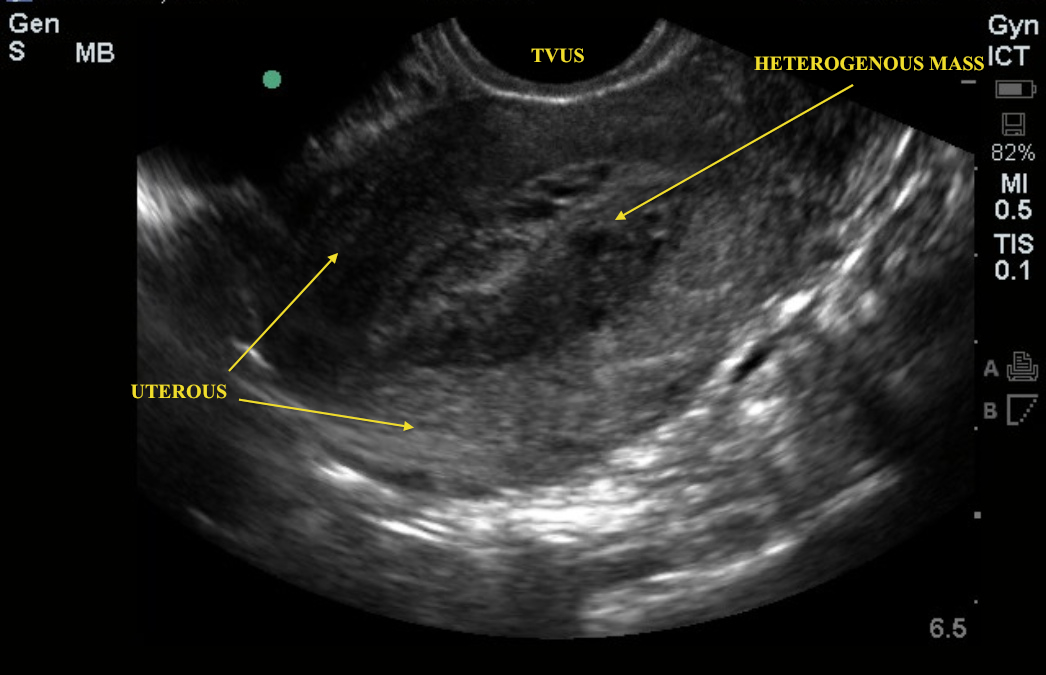
The video shows the uterus, using an intracavitary probe. Note the heterogeneous mass in the uterus. You do not see anything that looks like a classic intrauterine pregnancy. Notice the “grape-like” structures in the periphery. Bedside diagnosis – molar pregnancy.
Hydatidiform moles develop from an aberrant fertilization event that leads to the development of an abnormal proliferative process. Patients may have theca lutein cysts, hyperemesis gravidarum, and pre-eclampsia prior to 20 weeks gestation caused by abnormally high levels of ß-hCG. This patient had a ß-hCG of 8,500 with an unclear LMP. Although the ß-hCG is low in this case, let it be a reminder that not all patient pathology reads the medical literature on its classic presentation. Once a molar pregnancy is diagnosed, a baseline chest radiograph should be obtained, as the lungs are a primary site of metastasis for malignant trophoblastic tumors.
This patient was evaluated by GYN, underwent D&C, and had specimen sent to pathology for further evaluation.
Date: April 2013