This week’s image is a transverse suprapubic image with ultrasonographic evidence of small bowel obstruction in a patient with sigmoid volvulus.
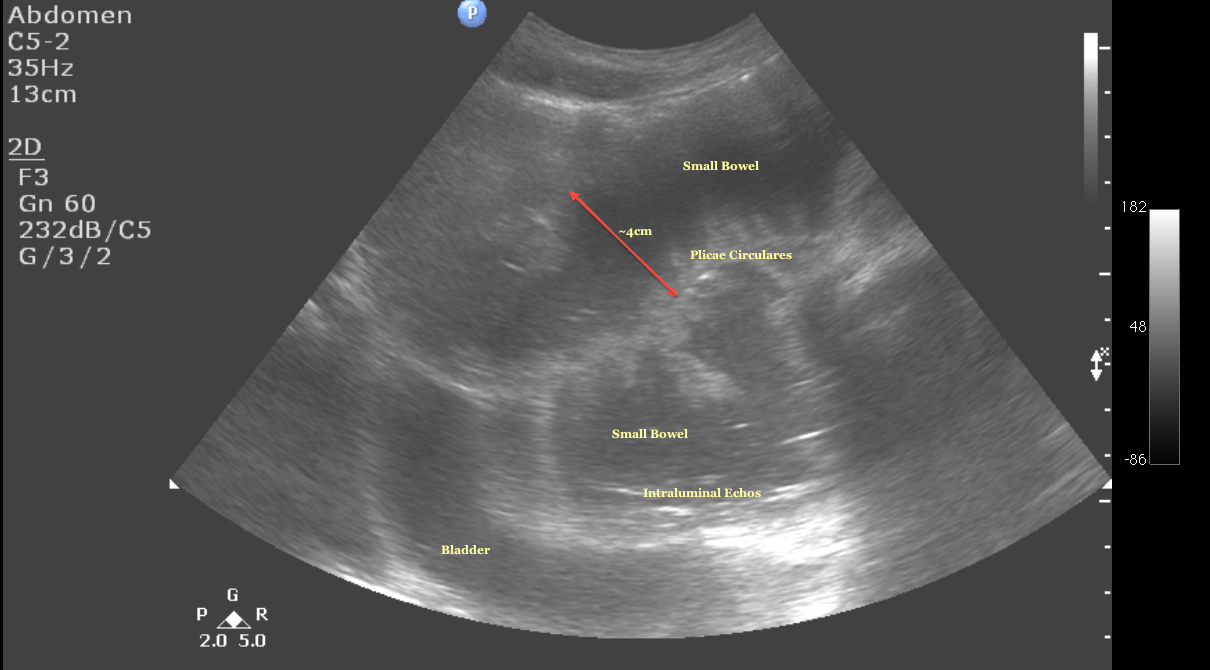
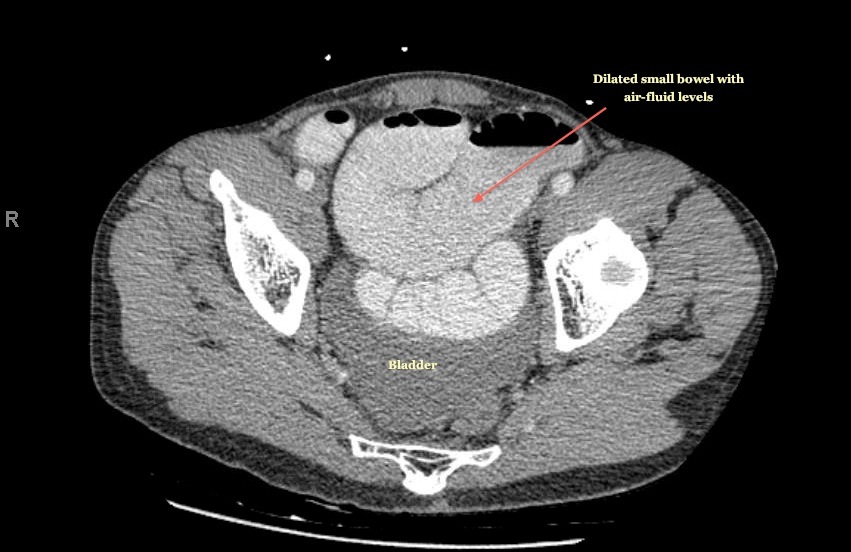
The view was obtained by placing the probe superior the pubic symphysis with the indicator toward the patient’s right side. There is also an attached image from the patients CT abdomen - look how closely these images resemble one another. Normally air within the lumen of bowel is a strong reflector of sound waves. This distorts the underlying anatomy. In obstruction, however, bowel is dilated and more fluid-filled, making the anatomy more accessible to ultrasound.
To diagnose SBO, look for fluid-filled, dilated loops of bowel (defined as >2.5cm) as seen here. You may also see back and forth movements of echoes within the bowel lumen as bowel contents move with dysfunctional peristalsis. The plicae circulares can be prominent as seen here. Diagnostic images can be obtained in the epigastric area, the bilateral colic gutters, or in the suprapubic abdomen. Remember air rises to the top so you may have more success finding fluid-filled loops in dependent areas, or by displacing gas by applying gentle pressure with the ultrasound probe.
Only a few small studies have looked point-of-care ultrasound for the diagnosis of SBO in the ED. After a 10-minute training session and 5 practice scans, residents at UCLA Olive View Medical Center were able to detect CT proven SBO with a sensitivity of 91% and specificity of 84% (Read the article). Small study with big confidence intervals, but the basic take-home message is that trained ED providers with an ultrasound are about as good as plain films. Something to try next time you are waiting for further imaging studies.