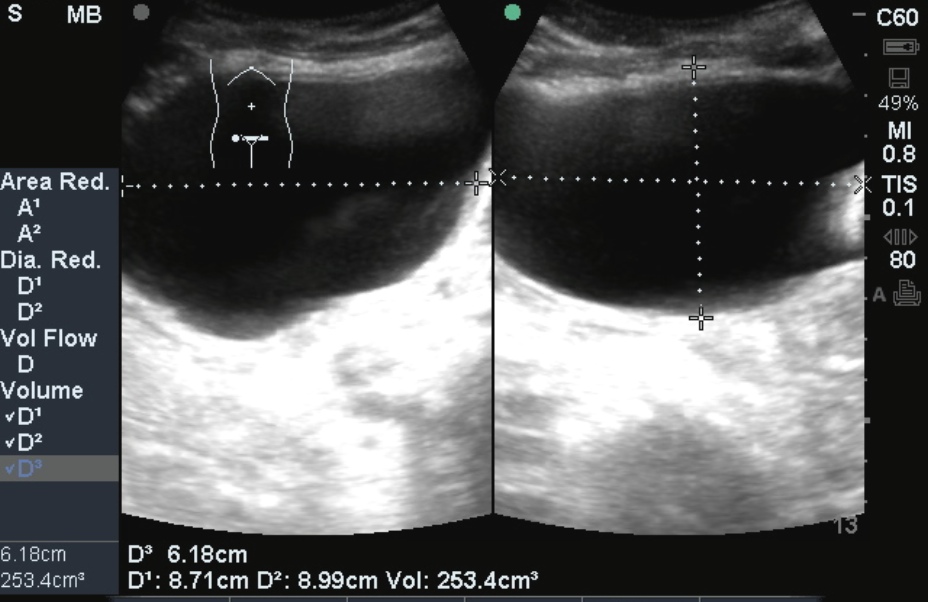
Who: A patient presented with post-obstructive hydronephrosis which was diagnosed using ultrasound (large bladder volume + hydronephrosis).
What: Severe Hydronephrosis
How: Start by placing the curvilinear probe with probe marker pointing to patient’s head on the patient’s right flank. This probe position will allow visualization of the kidney and liver, in what should be familiar as the Morrison’s pouch view of the FAST exam. Once the kidney is visualized, probe may be positioned and moved accordingly to improve visualization. Similarly, the left kidney may be visualized in the left flank, starting with the splenorenal view of the FAST exam and adjusting probe position to improve kidney visualization. Being retroperitoneal, kidneys are located posterior in the abdomen, and therefore best views are obtained with the probe closer to the posterior surface of the abdomen and with the sonographer’s hand lying on the bed. It is also best to evaluate in two planes: transverse and longitudinal. The technique described above assesses the kidney in it’s longitudinal axis and the horizontal view is located simply by rotating the transducer 90 degrees with probe marker oriented to the patient’s right side.
Hydronephrosis grading:
Normal: collecting system is collapsed and hyperechoic.
Mild: pelvis is open and filled with hypoechoic urine. Difficult to identify, however. Only dilation of the ureter may be seen.
Moderate: calyces are open with blunting.
Severe: calyces ‘ballooned’ out, pyramids/medulla obliterated, cortex remains.
Image 1
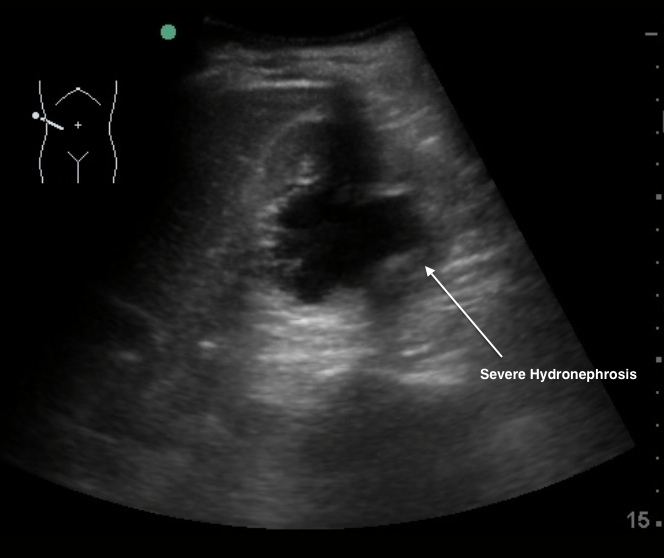
Image 2
Clinical Importance: Hydronephrosis may be acute and/or chronic. Urinary tract obstruction may lead to hydronephrosis. It is important to know the common medical terms used to describe the pathophysiology of urinary retention. The structural impediment to the flow of urine is termed obstructive uropathy. Unless this obstruction develops slowly it is typically painful, which is called renal colic. The most common cause is a kidney stone dislodged into the ureter called ureterolithiasis. Urine flow is blocked by the stone leading to backup and dilation of the proximal ureter (hydrometer). As the obstruction progresses, more proximal structures like the renal collecting system (renal pelvis and calyces) becomes dilated, termed hydronephrosis. If the hydronephrosis is severe, the renal parenchyma becomes compressed and if lasting long enough (about 2-4 weeks), can cause loss of renal function. Obstruction at or distal to the renal pelvis causes diffuse caliectasis or hydronephrosis. Ureteral obstruction may result from stones, transitional cell carcinoma, external compression (tumors, enlarged lymph nodes, retroperitoneal fibrosis), blood clots, and fungus balls. Bedside ED ultrasound is highly sensitive in detecting hydronephrosis.
Literature Support:
Henderson SO et al. Bedside emergency department ultrasonography plus radiography of the kidneys, ureters, and bladder vs intravenous pyelography in the evaluation of suspected ureteral colic. Acad Emerg Med. 1998 Jul;5(7):666-71.Dalziel PJ, Noble VE. Emerg Med J. 2013 Jan;30(1):3-8. Bedside ultrasound and the assessment of renal colic: a review.
Date: 2013