Small bowel obstruction with herniated bowel
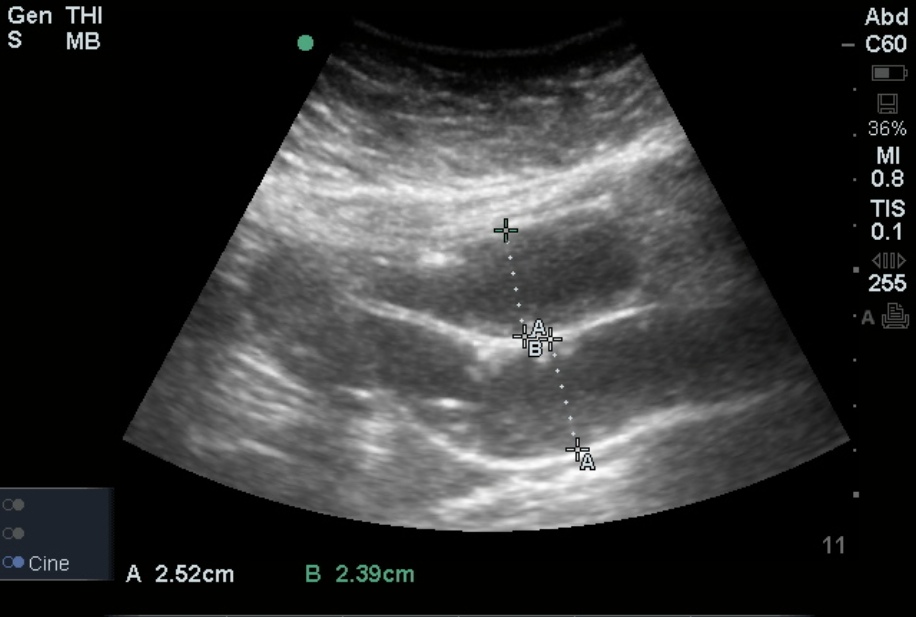
Abdominal scanning, including scanning for bowel, is performed best using the curvilinear probe. You may place the probe in the lower quadrants of the abdomen (fluid-filled loops will lie in dependent portions) or perform a methodical abdominal sweep starting the right upper quadrant and zig-zagging your way to the left lower quadrant. Dilated loops of bowel are visualized when there is a small bowel obstruction. The bowel is also noted to be fluid-filled with bidirectional dysfunctional peristalsis. When bowel diameter exceeds 2.5 cm, ultrasound diagnosis of obstruction is made. A defect in the linear hyperechoic fascia with bowel loops superior is suggestive of hernia.
Image 1: Hernia
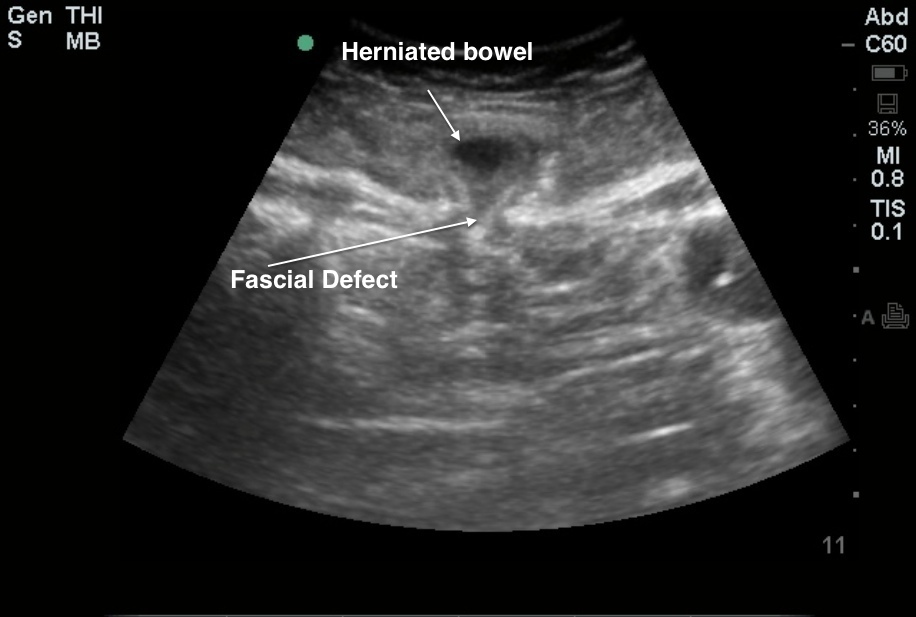
Image 2: SBO
Clinical Importance: CT is considered gold standard for detecting bowel obstructions (sensitivity/specificity ~ 92%/92%). However, ultrasound is equally apt at making the diagnosis (sensitivity/specificity ~ 88%/96%), much more so than the abdominal plain film (sensitivity/specificity ~ 70%/60%). A transition point may not necessarily be visualized using ultrasound, however. Additionally, dilated bowel loops should also prompt the diagnosis of ileus. Finally, in SBO, wall thickening may be prognostic and suggestive of IBD/colitis.
Literature Support: Suri et al. Comparative Evaluation of Plain Films, Ultrasound and CT in the Diagnosis of Intestinal Obstruction. Acta Radiol July 1999 vol. 40 no. 4 422-428
Date: 2014