This week’s image of the fortnight comes from a 5-week old male coming in with forceful nonbilious/non-bloody vomiting. The ultrasound findings are shown here:
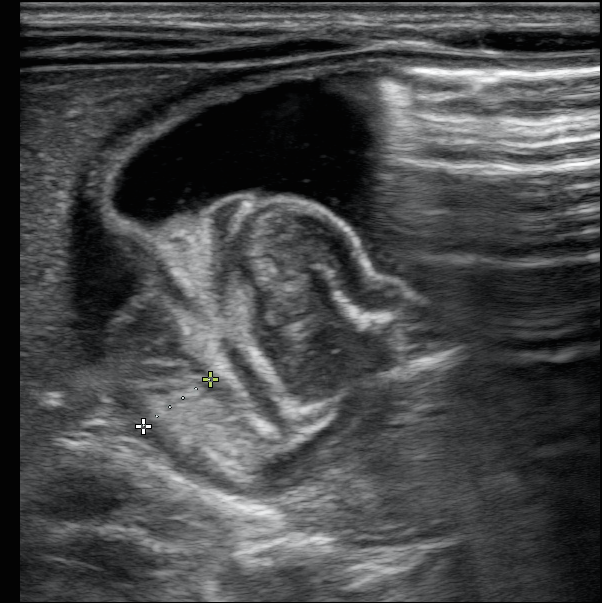
As you can see these of a thickened pylorus. This child was diagnosed with pyloric stenosis and taken to the operating room. The technique is to find the gallbladder, then turn the probe sagittally to find the pylorus longitudinally.
To diagnose pyloric stenosis remember π = 3.1415
This correlates to pyloric muscle thickness (muscular wall on transverse >3mm). Normal pylorus thickness is <2mm.
Pyloric Transverse diameter >12-14mm
Pyloric length > 15mm

As you can see on image 2, the antral nipple sign shows the redundant pyloric mucosa protruding back into the gastric antrum. Keep an eye on the pylorus. If the pylorus opens and contents pass through it, this excludes HPS. If there are issues with obtaining images, place the infant on left lateral decubitus and feed the child. Pylorus is medial to the gallbladder, lateral/anterior to the aorta.
Terry Singhapricha, M.D.
Emory Ultrasound Fellow
Reference:
Costa Dias S, Swinson S, Torrão H, et al. Hypertrophic pyloric stenosis: tips and tricks for ultrasound diagnosis. Insights into Imaging. 2012;3(3):247-250. doi:10.1007/s13244-012-0168-x.
Said M, Shaul DB, Fujimoto M, Radner G, Sydorak RM, Applebaum H. Ultrasound Measurements in Hypertrophic Pyloric Stenosis: Don’t Let the Numbers Fool You. The Permanente Journal. 2012;16(3):25-27.