The patient presented one week after a G-tube placement for RLQ abdominal pain and inability to tolerate tube feeds. The ultrasound image below was obtained in the RLQ at the patient’s point of maximal tenderness.
Image 1
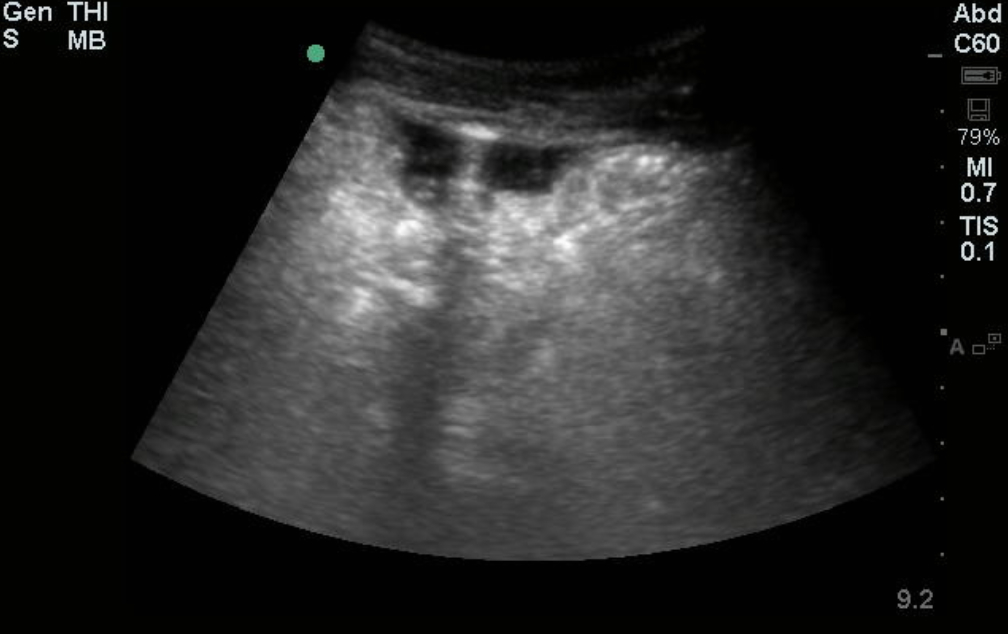
A large black, or anechoic, the area is seen just beneath the peritoneum. Notice that this area does not appear rounded like fluid within the lumen of a vascular structure, or within the bowel. Typically free fluid will form triangles as it fills the spaces between structures. Note that within the collection of fluid there is a smaller brighter area. To better visualize this they switched to the linear probe.
Image 2
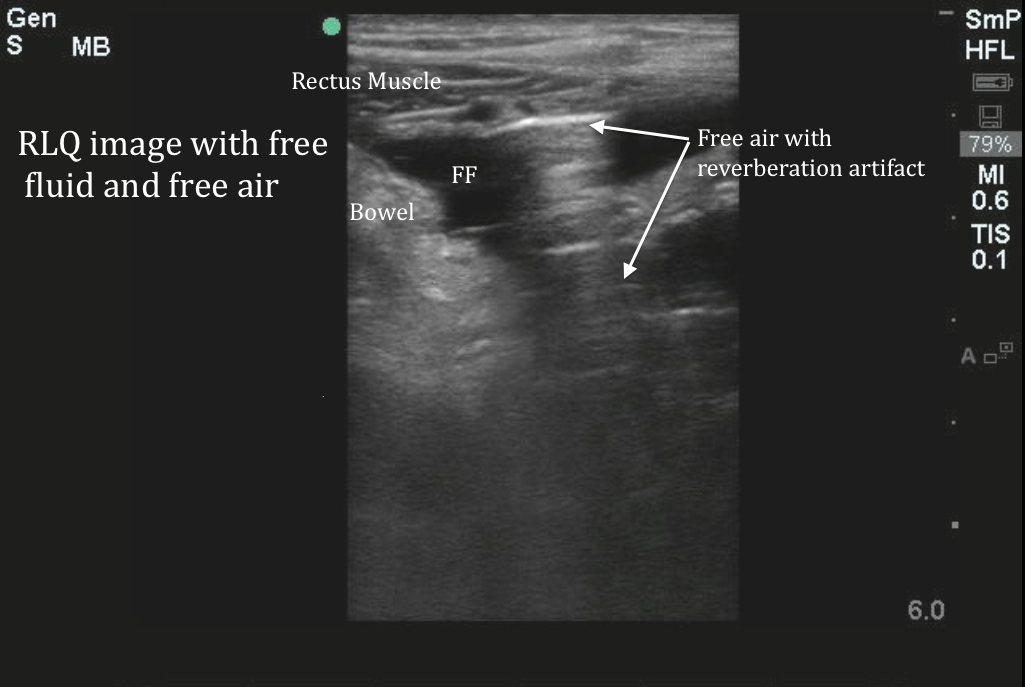
The free air in the image above looks similar to the A-line artifacts that we see when we image the lung. Free fluid outlines the air and makes it easier to see. In the absence of free fluid, pneumoperitoneum can be challenging to identify, as it is difficult to distinguish normal air within the intestines from pathologic free air. Free air will appear as ringdown or reverberation artifacts. It is typically best image over the ventral surface of the liver. Free air should easily move or change with compression of the probe. The air within the lungs, subcutaneous emphysema, and air within the GI tract can all be fake-outs for free air making this a challenging diagnosis. This patient was found to have gastric perforation and multiple intraabdominal abscesses and associated free air. They were taken to the OR for wash-out and repair of the perforation and did well.
Further Reading
Moriwaki, Y., Sugiyama, M., Toyoda, H., Kosuge, T., Arata, S., Iwashita, M., et al. (2009). Ultrasonography for the diagnosis of intraperitoneal free air in chest-abdominal-pelvic blunt trauma and critical acute abdominal pain. Archives of Surgery 1960, 144(2), 137–41
Date: 2014