Acute cholecystitis on ultrasound in the attached images. Please see image 1 - GB1 IOW and Image 2- GB2 IOW and the youtube link for a brief ultrasound clip of the pathology.
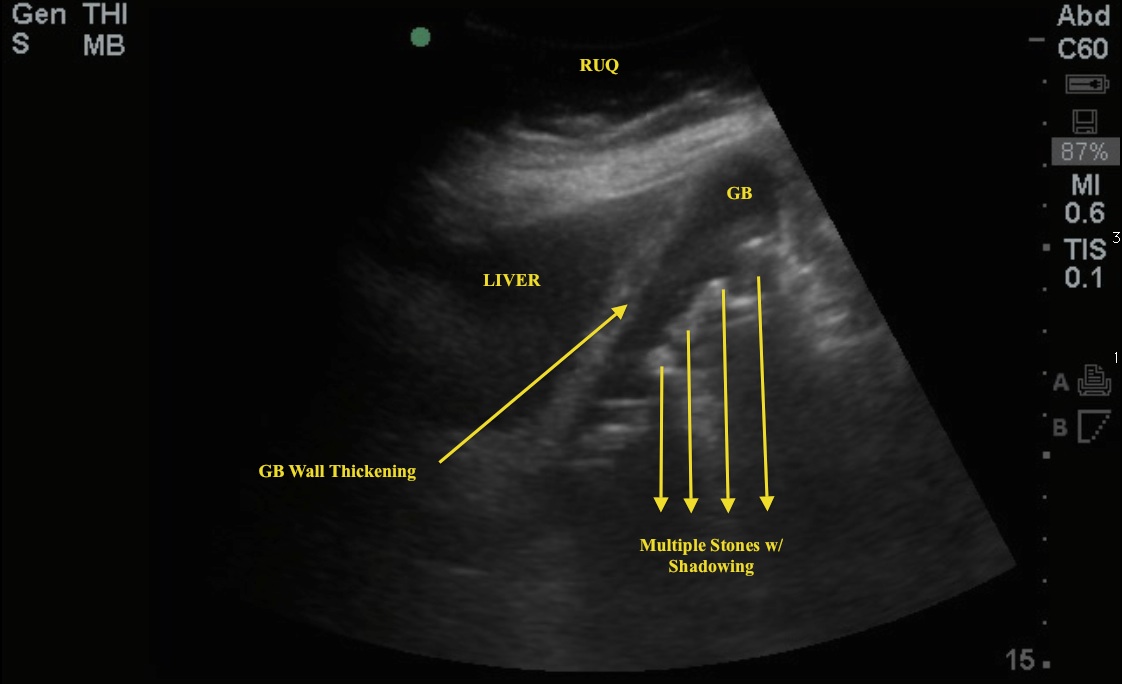
Image 1 - GB1 IOW
 .
.
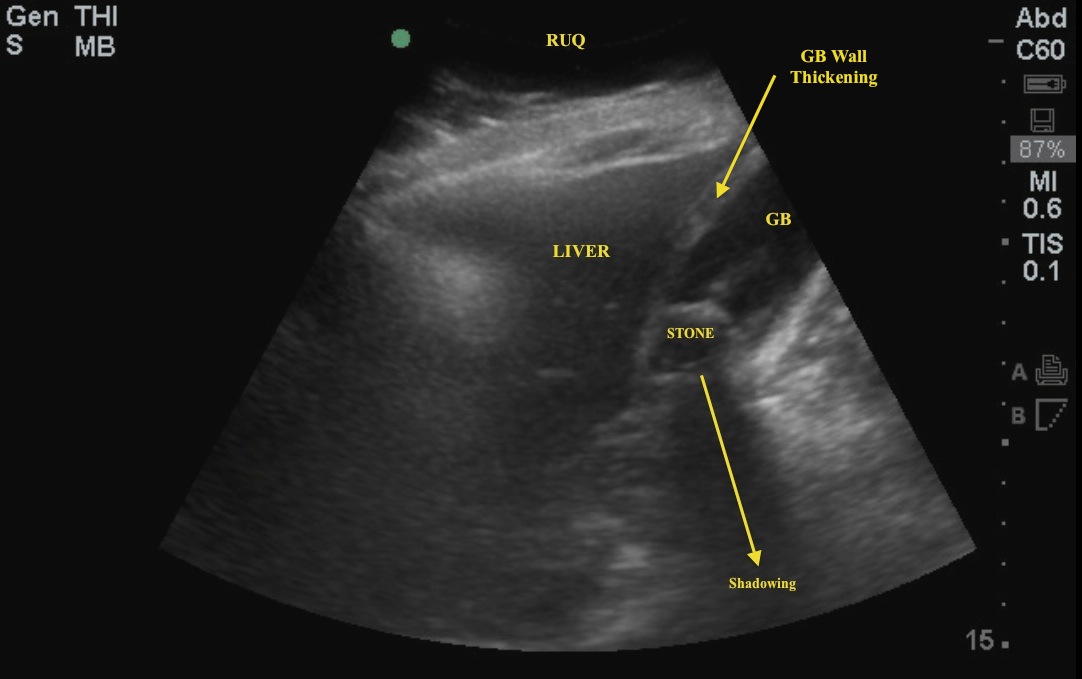
Image 2: GBI IOW2
 .
.
Ultrasound findings include the following:
- Cholelithiasis: Stones in the GB are hyperechoic, typically cause shadowing, and move when the patient changes position. Beware of falsely calling a polyp a stone! Polyps do not shadow, appear to be stuck to the GB wall and require followup to rule out malignancy.
- Gallbladder Wall Thickening: Normal measurement is <3mm. Make sure to measure this on the anterior wall! Posterior acoustic enhancement can often distort the posterior wall measurement and make it appear falsely enlarged. Note also that the GB wall can appear thickened after a patient consumes a fatty meal. This is normal and the patient typically has no other signs of cholecystitis (i.e., ultrasonic Murphy's sign or PCF). Another instance of GB wall thickening is when the patient has generalized edema (i.e., liver failure). This can cause edema of the GB wall as well.
- Pericholecystic Fluid (PCF): Serous fluid that accumulates as a result of an inflamed gall bladder wall.
- Ultrasonic Murphy's sign: Tenderness upon compressing the GB with the probe. This is often operator-dependent.
Although this is not required to make the diagnosis of cholecystitis, the common bile duct is often evaluated when looking at the gall bladder for possible stone. An enlarged CBD indicates an obstruction. Normal measurement is <4mm with an extra 1mm allowed for every decade in age over 40. Note also that CBD is also enlarged after a cholecystectomy since the CBD becomes the default reservoir for bile.
February 2013